Today
Many put the start of the quality revolution with the NBC Television’s show “NBC White Paper.” On June 24, 1980 Lloyd Dobbins introduced W. Edwards Deming to America in an episode entitled: If Japan can… Why can’t we?
The show addressed how Deming’s advice on continuous process improvement and recognizing that manufacturing is a system, not simply separate assembly steps. While the application of what came to be called TQM was applied sporadically within healthcare, the use of PDCA seemed to take hold and became widespread in its use. Not only did it align nicely with the scientific method widely understood in healthcare, but gained momentum when it was modified with the addition of the set of preliminary steps: FOCUS, by Hospital Corporation of America (currently the largest private operator of health care facilities in the world). It is not known whether the expansion of its use was based on efficacy or the notoriety of its developer.
While many quality theories or approaches were short-lived, three seemed to take hold—albeit independent of each other. Starting in manufacturing, these three methods have survived to improve quality and efficiency: Lean, Six Sigma, and Constraints Management. Throughout the 1990s, these methodologies began to be applied in other industries. Despite successes wherever applied, certain industries have been slower to accept certain quality tools and methods from manufacturing despite more than 30 years of successful application. It is critical to note that the finding is about acceptance, not applicability; for example, while control charts have been used extensively in manufacturing since the 1920s and have been used successfully in healthcare, their usage is not as widespread as one would expect.
Lean in Healthcare
Lean focuses on eliminating waste. Most literature lists seven different types of waste (shown below). While these were developed originally for applicability within manufacturing, they are equally relevant in healthcare.
Transport. Any time people, materials, or information must be moved, it is defined as waste. Moving patients from room to room is an example of waste. While in many cases necessary, this transportation nonetheless is viewed as waste. Use of a spaghetti diagram may help to minimize this type of waste.
Inventory. While it is necessary to maintain inventories to ensure availability, anything short of just-in-time (JIT) availability is categorized as waste. Tools such as kanban can mitigate this kind of waste.
Motion. A nurse’s station with a desktop computer at one end and a printer at the other that requires nurses to move excessively to pick up printouts is an example of waste. Good ergonomic practices and more efficient workspace layouts can moderate this waste.
Waiting. This waste is endemic to healthcare. We even call our primary customers patients—is this because it is an expectation? Elimination of non-value-adding activities can diminish this waste.
Overproduction. Running too many tests and printing too many copies of paperwork are examples of overproduction. Reviewing standard lab panels or pursuing paperless processes can mitigate this type of waste.
Overprocessing. Requiring excess approvals and running the same test twice are examples of overprocessing. The elimination of non-value adding activities can lessen this sort of waste dramatically.
Defects. When a product or service does not meet specification or customer expectations, it is a defect. Defects often result in rework, and the associated costs frequently go unaccounted for.
Six Sigma in Healthcare
The power of Six Sigma is its ability to identify root causes of complex problems and reduce variation, both of which are central to the improvement of processes. Examples of Six Sigma applications in healthcare include reduction of infection rates, patient falls, and missed appointments, as well as enhanced medication reconciliations and coding. Anywhere the root cause is not known. While historically, the concept of root cause analysis in healthcare process improvement has relied largely on softer tools such as Failure Modes and Effects Analysis and Fishbone Diagrams; Six Sigma relies on the use of inferential statistics to validate root causes.
Constraints Management in Healthcare
Constraints Management is a management philosophy encompassing an integrated suite of techniques used in operations and supply-chain management, project management, conflict resolution, and strategic planning. Dr. Eliyahu Goldratt began its development in 1979 with the production scheduling software OPT, and has led its evolution into three interrelated areas—logistics/production, performance measurement, and problem-solving/thinking tools.
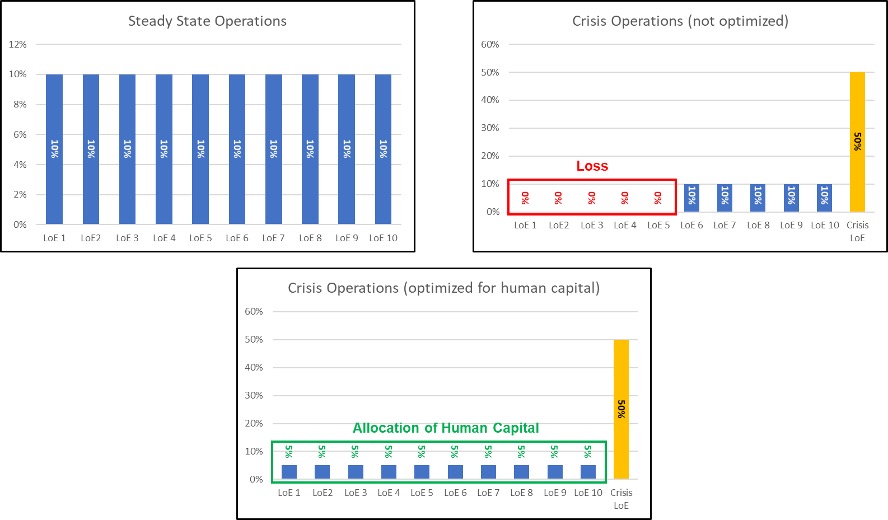
It is a systematic approach to managing complex organizations by identifying and controlling key leverage points within a system or process. By managing these key control points, healthcare organizations can focus on areas that drive system-level improvement instead of trying to manage every element of a process, which can lead to local optimization without systemic impact.
A constraint is anything that limits the system from achieving higher performance relative to its goal. In healthcare, a constraint is anything that impedes the ability or means to provide or deliver care. Common types of constraints include:
- Market
- Resource
- Material
- Supplier/vendor
- Financial
- Knowledge/competence
- Policy
Once the constraint is identified, numerous tools are available to mitigate it. Within healthcare, Constraints Management was pioneered at the University of Pretoria Medical School in 1991. One of the earliest reported applications of Constraints Management in U.S. healthcare was at the University of Michigan Hospital. The hospital’s admission and discharge system was inefficient, resulting in an average of three hours’ delay in accepting incoming patients, who waited for their rooms to be prepared. Constraints Management allowed the hospital to reduce the average time to admit patients from 3 hours to just 11 minutes.
Transition to an Integrated Approach
Each of these methodologies has stood the test of time; each has been around as a distinct entity for more than 30 years. The problem is that most people tend to be in one camp or another. After years or practice and much research, we (NOVACES) have come to the—not so shocking—conclusion that one should apply the right tool to the right problem at the right time.
If you are looking for focus: you might look in the Constraints Management section of your toolbox, root cause analysis: Six Sigma section; improving flow: the Lean section. Maybe even sometimes, you might have to pull something from a couple of sections to solve the same issue!